"I think I have a heel spur" is one of the most common things patients tell me when they walk through the door at VitaStep Podiatry. They've Googled their heel pain, seen an image of a bony protrusion on an X-ray, and concluded that a sharp calcium spike is the villain causing their suffering. The reality is more nuanced — and understanding it is the difference between getting the right treatment and spending months pursuing the wrong one.
What Is Plantar Fasciitis?
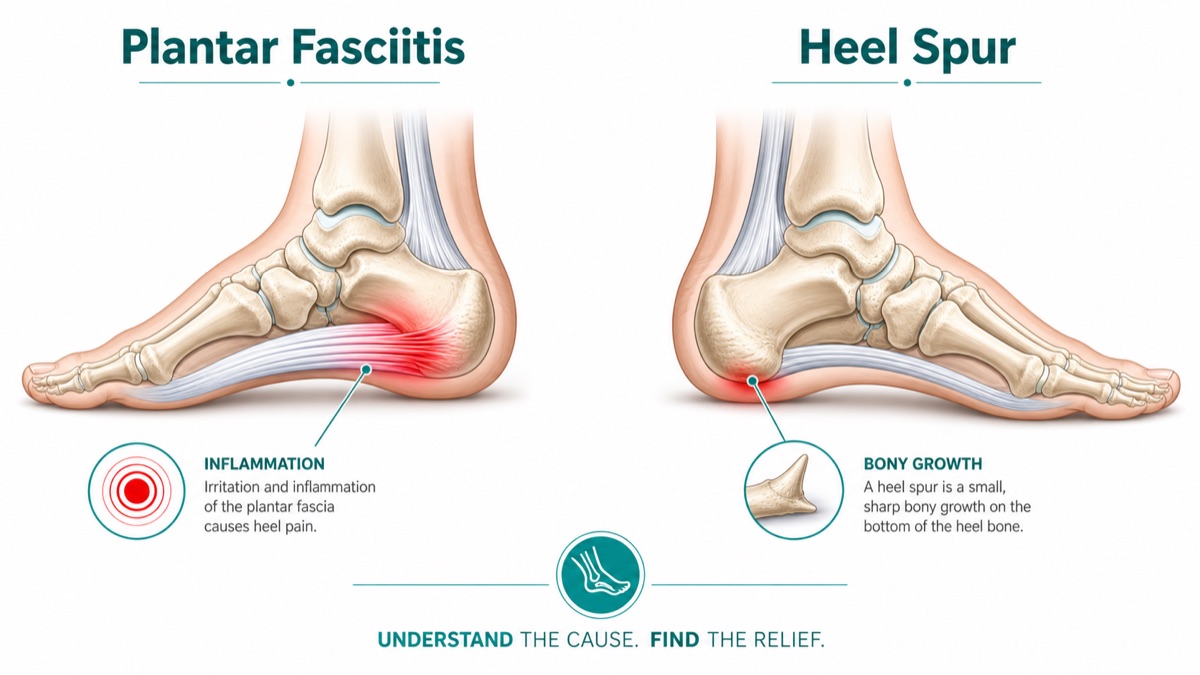
Plantar fasciitis (technically, plantar fasciopathy in modern clinical terminology) is inflammation and micro-tearing of the plantar fascia — the thick fibrous ligament that spans the bottom of your foot from the heel bone to the base of your toes. It functions as a structural bowstring, supporting your arch and absorbing impact with every step. When the fascia is repeatedly overloaded — by excessive running, prolonged standing, inadequate footwear, sudden weight gain, or biomechanical factors like high arches or flat feet — it develops small tears at its origin point on the calcaneus.
The body responds to these micro-tears with an inflammatory cascade. Over time, if the injury-repair cycle is repeatedly disrupted, the tissue undergoes degenerative changes (fasciosis) rather than true healing. This is why plantar fasciitis that is left untreated often becomes a chronic condition lasting a year or more.
Plantar fasciitis is not visible on X-ray. It is a soft-tissue injury. The diagnosis is clinical — based on the location and character of your pain, physical examination findings (tenderness at the medial calcaneal tubercle), and, when needed, musculoskeletal ultrasound to measure fascial thickness and detect partial tears.
What Is a Heel Spur?
A heel spur is a calcium deposit — technically a traction osteophyte — that forms at the point where the plantar fascia attaches to the calcaneus. It develops in response to chronic traction stress: when the fascia repeatedly tugs on the periosteum (the bone's outer membrane), the body lays down calcium to reinforce the attachment site. The result is a bony projection, sometimes hook-shaped, that is visible on an X-ray.
Here is the critical clinical fact that surprises most patients: approximately 50% of people with plantar fasciitis have a heel spur, but so do roughly 15–25% of people with no heel pain whatsoever. The spur is a consequence of chronic fascial stress — a radiographic marker of past and ongoing traction — not a knife-like protrusion that independently stabs your heel with every step. Cadaveric studies have shown that these spurs are actually located within the intrinsic foot musculature, not in the plantar fascia itself.
The key distinction: Plantar fasciitis is the cause of your pain. A heel spur is a result of long-standing plantar fasciitis — and in most cases, it is clinically silent. Treating the spur without treating the fascia accomplishes nothing.
How Are They Diagnosed?
At VitaStep, the diagnostic workup for heel pain typically proceeds as follows:
- History and symptom review: When does it hurt? Where exactly? What makes it worse? Is it morning pain that improves with walking? Has there been a recent change in activity or footwear? A detailed history rules out inflammatory arthritis, nerve entrapment, and other conditions that can mimic plantar fasciitis.
- Physical examination: Palpation of the medial calcaneal tubercle reproduces the classic plantar fasciitis pain. We also assess ankle dorsiflexion range of motion (restricted dorsiflexion is a major risk factor), evaluate arch height and foot mechanics, and perform the windlass test to assess plantar fascial tension.
- X-ray: We order weight-bearing foot X-rays to identify heel spurs, assess bone structure, rule out stress fractures, and evaluate joint alignment. The presence or absence of a spur on X-ray informs diagnosis but does not change the initial treatment approach.
- Musculoskeletal ultrasound: When the diagnosis is unclear or we want objective data on fascial thickness (normal is <4 mm; plantar fasciitis typically shows >4–5 mm), in-office ultrasound provides real-time imaging without radiation. It also identifies partial tears and guides precise injection therapy.
- MRI: Reserved for cases where a stress fracture, nerve entrapment (Baxter's nerve), or soft-tissue mass is suspected. Not routinely required for plantar fasciitis diagnosis.
Treatment: Plantar Fasciitis First, Spur Last
The treatment hierarchy for both conditions begins the same way — because addressing plantar fasciitis is what resolves the pain, regardless of whether a spur is present.
Conservative Treatment (First-Line)
- Stretching protocol: Plantar fascia-specific stretches and Achilles/calf stretching, performed consistently 2–3 times daily, remain the cornerstone of plantar fasciitis management.
- Custom prescription orthotics: Unlike over-the-counter insoles, prescription orthotics are fabricated from a digital scan of your foot and designed to address your specific biomechanical deficiencies — whether that is controlling excessive pronation in flat feet or offloading the fascial insertion in a high-arched foot.
- Night splints: Keeping the foot in dorsiflexion during sleep prevents the overnight fascial contracture that causes severe morning pain.
- Activity modification and footwear: Temporary reduction in high-impact activity combined with a transition to supportive footwear with adequate heel cushioning.
Intermediate Interventions
- Corticosteroid injection: A precisely placed injection at the fascial insertion delivers potent anti-inflammatory medication directly to the site of pathology. It provides significant short-term pain relief — often within days — and can break the pain-inflammation cycle that perpetuates the condition. Ultrasound-guided injection improves accuracy and reduces the small risk of fascial rupture from repeat injections.
- Extracorporeal shockwave therapy (ESWT): For chronic plantar fasciitis (lasting more than 6 months), ESWT delivers focused acoustic energy to the fascial insertion, stimulating tissue remodeling and neovascularization. Research shows 70–80% success rates for chronic cases resistant to other conservative measures. It requires 3–5 sessions and is generally well-tolerated.
- Physical therapy: A structured program targeting calf flexibility, ankle dorsiflexion, intrinsic foot strengthening, and gait retraining accelerates recovery and prevents recurrence.
Surgical Treatment (Last Resort)
Surgery for plantar fasciitis is considered only after 6–12 months of documented, consistent conservative treatment has failed. Most insurance carriers require this threshold. The primary procedure is a partial plantar fascia release — severing the tightest portion of the fascial band to relieve chronic tension at the calcaneal insertion. This can be performed endoscopically (through two small portals, 5–7 mm each) with a recovery of 4–6 weeks.
Heel spur removal (calcaneal exostectomy) is occasionally performed at the same time as a fascial release, particularly when the spur is large and contributing to local soft-tissue irritation. However, it is never performed as a standalone procedure for pain relief. The fascia — not the spur — is the pain generator.
What This Means for Escondido's Active Community
Escondido and the surrounding North County San Diego area have an exceptionally active population. Hikers, trail runners, youth sports families, and outdoor enthusiasts who use the local trail networks around Lake Dixon, Daley Ranch, Dixon Lake, and the Kit Carson Park system put significant cumulative load on their feet. Early diagnosis of plantar fasciitis — before a heel spur has had time to form — means a shorter treatment course, less disruption to your active lifestyle, and a much lower chance of requiring injections or surgery.
If you have been told you have a heel spur, or if you are experiencing the classic morning heel pain described in this article, the most important next step is a proper podiatric evaluation. An X-ray finding of a spur should not send you directly to a surgeon — it should send you to a podiatrist who will treat the fascia first and monitor your progress. At VitaStep Podiatry, we see new heel pain patients within days, not weeks.